

Modern PRN staffing platforms allow facilities and nurses to match shift needs in real time, reducing the strain on both sides
More than half of U.S. nurses reported burnout in 2024. Not as a vague feeling of exhaustion, but as a clinical syndrome now linked by peer-reviewed research to higher rates of medication errors, patient falls, and hospital-acquired infections.
At the same time, the nursing workforce is shrinking. Over 138,000 nurses exited the profession between 2022 and 2024, and projections from the National Council of State Boards of Nursing (NCSBN) suggest nearly 40% of currently practicing nurses intend to leave by 2029.
These two facts aren’t separate crises. They’re the same crisis, looping back on itself. Burned-out nurses leave. Fewer nurses means heavier workloads for those who stay.
Heavier workloads produce more burnout. The solution the industry has reached for – pay nurses more, recruit harder, import internationally – hasn’t broken the cycle because it doesn’t address what’s actually driving people out.
PRN nursing offers something different. Not a recruitment shortcut, but a structural shift in how nurses relate to their work. The psychology behind why it works is worth understanding, whether you’re a nurse wondering if it fits your situation or a facility administrator rethinking your staffing model.
What PRN Nursing Actually Means (and Why the Terminology Matters)
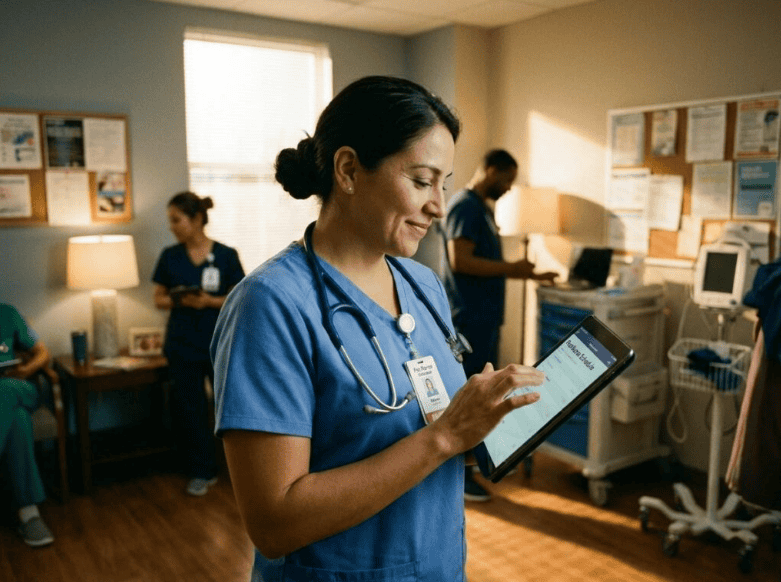
A nurse using a PRN staffing platform to choose her own shifts – a growing solution to the rigid scheduling that fuels burnout
PRN comes from the Latin “pro re nata,” meaning “as needed.” In practice, PRN nurses work on a scheduled-as-needed or on-call basis, filling coverage gaps without the contractual commitment of full-time or part-time permanent roles. Hospitals, long-term care facilities, and outpatient clinics all use PRN arrangements to handle census fluctuations, planned leave coverage, and unexpected absences.
It’s worth distinguishing PRN from per diem, because the terms get used interchangeably and they’re not quite the same thing. PRN nurses typically work within a single facility and may have some degree of shift predictability. Per diem nurses generally float across multiple facilities through staffing agencies, often with no guaranteed hours at all. The psychological benefits of both models are similar – schedule control, reduced mandatory overtime, and lower institutional dependency – but the logistics differ.
Technology has made this model far more practical than it was a decade ago. Platforms built around this need, like this PRN nurse staffing solution from Nursa, allow facilities to post open shifts and qualified nurses to claim them on their own timeline, without the friction of agency middlemen or the rigidity of traditional float pools.
One underappreciated benefit for PRN nurses: they tend to sidestep the cognitive and emotional toll of administrative overload that full-time staff absorb daily. When you’re not a permanent employee, the committee meetings, the documentation backlogs, and the institutional politics that drain psychological resources aren’t your problem in the same way.
The Psychological Toll of Full-Time Nursing: Burnout by the Numbers
The contrast between chronic overwork in fixed nursing roles and the recovery space that flexible scheduling can provide
Burnout in nursing is usually analyzed through the Maslach Burnout Inventory framework: emotional exhaustion, depersonalization (treating patients as objects rather than people), and a reduced sense of personal accomplishment. These aren’t just feelings. They’re measurable psychological states with documented downstream effects.
The scale of the problem in 2025 is hard to overstate. AMN Healthcare’s 2025 Survey of Registered Nurses, which drew responses from over 12,000 nurses, found that 58% feel burned out most days and 64% say compassion fatigue has affected their physical health. IntelyCare’s 2024 nursing survey, with over 5,000 respondents, put the figure even higher: 75.8% of nurses experienced burnout in 2023, and only 6.9% said they had never felt burned out at all.
The patient safety consequences are well-documented. A 2024 meta-analysis published in JAMA Network Open, drawing on 85 studies involving 288,581 nurses, found that burnout was directly associated with increased medical errors, patient falls, nosocomial infections, and reduced patient satisfaction. That’s not a correlation buried in a footnote. It’s a systematic review linking nurse burnout directly to patient harm.
What drives burnout at this scale? The CDC’s National Institute for Occupational Safety and Health (NIOSH) has identified the key risk factors for healthcare worker burnout as unpredictable long hours, high administrative burden, insufficient staffing, and – critically – little control over work schedules. These aren’t peripheral complaints. They’re the structural features of most full-time hospital nursing positions.
How PRN Staffing Addresses the Psychological Roots of Burnout

Facilities that use flexible PRN staffing models tend to report better-rested nursing teams and stronger staff morale
The psychological case for PRN nursing starts with Self-Determination Theory, developed by Edward Deci and Richard Ryan at the University of Rochester. The theory identifies three core psychological needs that, when met, sustain motivation and wellbeing: autonomy, competence, and relatedness. When any of these needs is chronically frustrated, the result is disengagement, exhaustion, and eventually exit.
For nurses in traditional full-time roles, autonomy is the first casualty. Mandatory overtime, involuntary float assignments, back-to-back shifts without adequate recovery – these conditions systematically undermine the sense of control that SDT identifies as essential to psychological health.
PRN nursing restores that control. Nurses choose which shifts they accept. They can decline work when they’re depleted. They can protect recovery time, preventing cumulative exhaustion from becoming clinical burnout. A 2025 national survey of 2,600 nurses and nursing students, published in Science Daily in April 2025, found that 55% strongly agreed flexible scheduling would improve their working environment.
There’s also a case for variety as a burnout prevention strategy. Rotating across units or facilities – rather than repeating the same high-stress environment every week – disrupts the monotony-driven emotional exhaustion that psychologists have identified as distinct from acute overwork burnout. Some nurses report that exposure to different teams and patient populations keeps clinical work feeling meaningful in ways a single unit can’t sustain over the years.
The broader mental health ecosystem matters here, too. PRN flexibility works best when nurses also have access to employee assistance programs and structured mental health supports that address burnout’s psychological roots directly. Schedule flexibility and clinical counseling aren’t competing strategies – they work better together.
What the Nursing Shortage Means for Facilities – and Why PRN is a Strategic Response
The shortage isn’t a future concern. It’s the current operating reality for most hospitals. The NCSBN’s data shows 138,000+ nurses have already left the workforce since 2022. The U.S. Bureau of Labor Statistics projects 194,500 open RN positions per year through 2034, and the total shortage is expected to reach 250,000 registered nurses by 2030.
For facilities, the financial pressure is real. The per diem nurse staffing market generated $4.36 billion in revenue in 2023 and is projected to grow to $6.36 billion by 2030 at a compound annual growth rate of 5.5%, according to Grand View Research’s 2024 industry analysis. That growth reflects how hospitals are already responding: not by filling permanent roles they can’t fill, but by building flexible staffing capacity to handle coverage gaps without overloading permanent staff.
The psychological angle here matters specifically for administrators. Burned-out permanent staff doesn’t just cost you in morale – they leave. NSI National Health Care’s 2024 Retention Report put average hospital RN turnover at 16.4% in 2023. Each departure costs a hospital an estimated $40,000 to $64,000 to replace, factoring in recruitment, orientation, and the productivity gap during transition. A PRN pool that keeps staffing ratios manageable isn’t just an operational convenience; it protects the psychological sustainability of your permanent staff.
Workforce strain also has a ripple effect that reaches patients before they even walk through the door. When nurses are burned out, and facilities are understaffed, the experience of care deteriorates in ways that contribute to patterns of healthcare avoidance that researchers have now begun to document at scale.
The AMN Healthcare 2025 Survey of Registered Nurses makes a useful point here: nurses aren’t just leaving because they’re tired. They’re leaving because they don’t believe the conditions will change. Facilities that build credible structural alternatives – including real PRN programs with adequate pay and shift availability – send a different message.
The Real-World Psychology of Choosing PRN: Who Benefits Most
PRN work isn’t right for every nurse at every stage of a career. But the populations where it tends to work well are broader than most people assume.
New nurses entering a fragmented healthcare system often find that PRN or per diem work provides exposure across settings that a single full-time position can’t offer. The tradeoff is a higher cognitive load (new environments require more vigilance), but many early-career nurses report it accelerates their clinical confidence in ways that sitting on one unit for two years doesn’t.
Nurses recovering from burnout are perhaps the most compelling use case. Re-entering practice after a period of exhaustion or leave through a PRN arrangement – working two or three shifts per week on your own terms – allows gradual re-engagement without triggering the same overload that caused the exit. It’s a genuine step-down model, not just a scheduling accommodation.
Nurses with caregiving responsibilities at home report that schedule flexibility aligns their professional work with family demands in ways that fixed scheduling never could. For this group, the alternative to PRN isn’t full-time nursing – it’s leaving the profession entirely.
Near-retirement nurses who want to stay engaged clinically without the physical and psychological demands of full-time work get a sustainable on-ramp. The American Nurses Association frames per diem work as a legitimate career choice aligned with nurses’ personal goals – not a lesser or temporary option.
The Limitations Worth Knowing
PRN nursing isn’t frictionless. The drawbacks are real and worth naming directly.
Income unpredictability is the biggest one. Without guaranteed hours, financial stress can replace scheduling stress – and for nurses supporting families or managing student debt, that’s not a neutral trade. Pure per diem arrangements with no shift minimums can leave nurses scrambling during slow census periods.
Most PRN and per diem roles don’t include employer-sponsored benefits. No health insurance, no retirement contributions, no paid time off. Nurses who take this route need to budget for those costs independently, which adds a different layer of financial planning that full-time employment handles automatically.
Social isolation is a more subtle risk that doesn’t get enough attention. Permanent staff build team cohesion and informal support networks that are genuinely protective against burnout. PRN nurses who float across units or facilities don’t build those bonds in the same way. Research consistently shows that social support at work buffers psychological strain, and PRN nurses may have less of it.
Finally, less experienced nurses may find that PRN settings are stressful precisely because of limited orientation and onboarding. Walking into an unfamiliar unit and being expected to function independently from day one requires a level of clinical confidence that takes time to build.
These are manageable limitations, not disqualifying ones. But anyone advising nurses – or making staffing decisions as an administrator – should address them directly rather than treating PRN as a universal answer.
Rethinking Staffing as a Psychological Intervention
The nursing burnout crisis has produced a lot of conversation about resilience training, wellness apps, and mental health resources – all of which have a place. But none of them changes the conditions that produce burnout in the first place.
PRN nursing does. Not perfectly, and not for everyone. But it directly addresses the three psychological drivers that clinical research consistently identifies as precursors to burnout: lack of autonomy, unsustainable workload, and eroded work-life boundaries.
The nursing shortage won’t be solved by recruiting more people into conditions that push existing nurses out. The profession needs structural changes that make sustained careers psychologically viable. For some nurses, that means finding a full-time position with genuine schedule flexibility. For others, it means stepping into PRN work and treating schedule control as a non-negotiable professional need rather than a luxury.
For facilities, the question worth sitting with is this: what does your current staffing model do to the psychological health of your permanent nurses? If the honest answer involves chronic understaffing, mandatory overtime, and high turnover, a serious PRN strategy isn’t a workaround. It’s part of the fix.